5 Signs Your Dispatch Process Is Costing You Revenue
If your dispatchers are the only ones who know what's happening in the field, you have a problem. Here are five warning signs that your dispatch process is leaking revenue.
Dispatch is the heartbeat of any DME field operation. When it works well, patients get served on time, technicians stay productive, and revenue flows. When it breaks down, the problems compound quickly, but they often stay invisible until the damage is already done. Here are five signs that your dispatch process is quietly costing you money.
1. You Find Out About Problems at the End of the Day
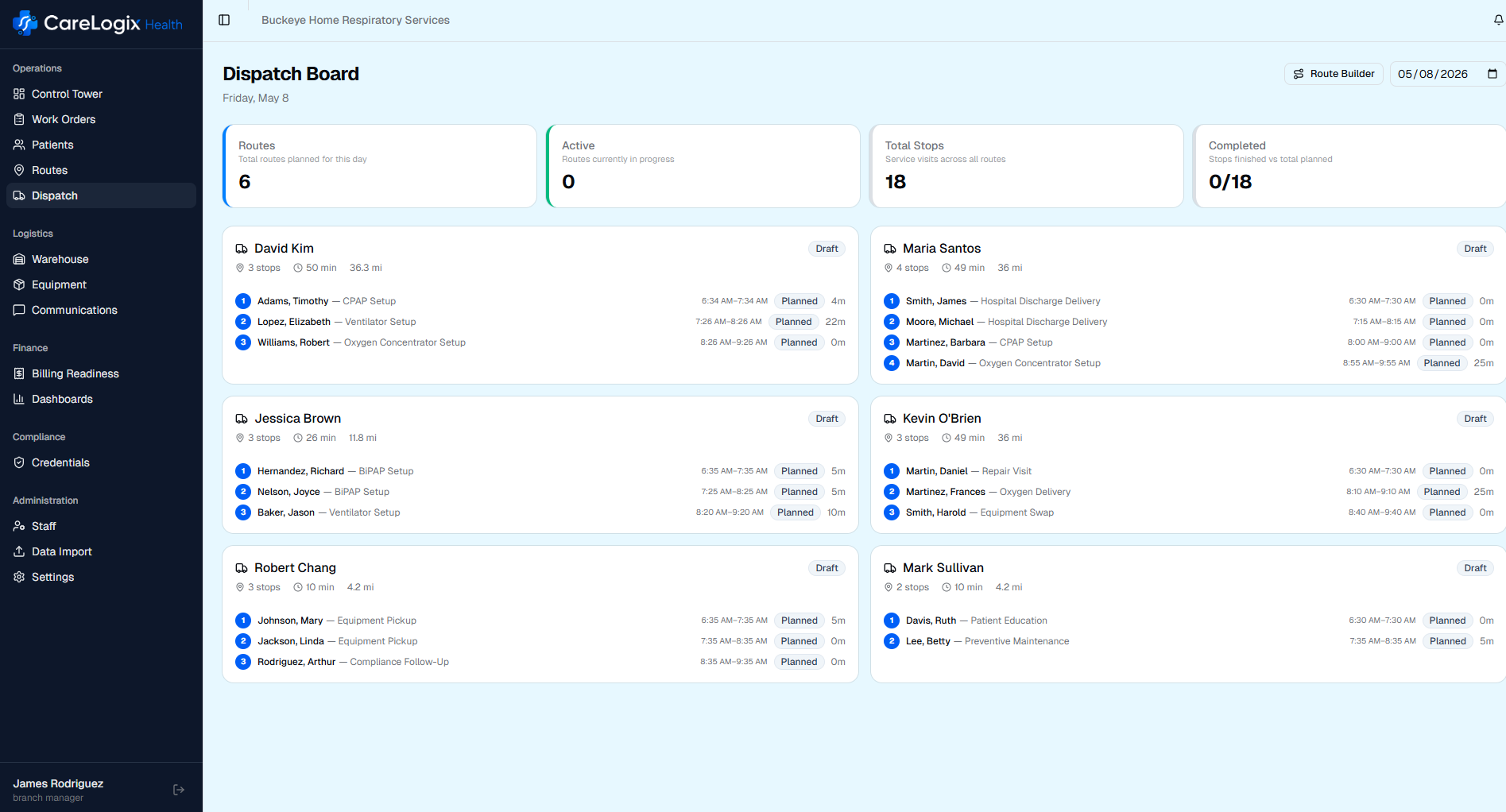
If your primary mechanism for learning about field issues is the end-of-day debrief, or worse, the next morning's review, you're operating blind during the hours when problems can still be fixed. A missed delivery window at 10 AM can often be recovered by 2 PM if someone knows about it. Discovered at 5 PM, it becomes a reschedule, an unhappy patient, and potentially a missed billing window.
Real-time visibility into field operations isn't a luxury. It's the difference between recovering from a disruption and absorbing its full cost. If your dispatch team can't see, in real time, which stops have been completed, which are running late, and which are at risk, you're flying blind.
2. Technicians Are Calling Dispatch for Directions
This might sound minor, but it's a symptom of a deeper problem. When technicians have to call dispatch to ask where they're going next, to confirm a patient address, or to get details about the equipment they're delivering, it means information isn't flowing to the field automatically.
Every inbound call to dispatch takes a dispatcher away from managing exceptions and monitoring the operation. If your dispatchers are spending 30% of their day answering basic informational questions from the field, they don't have capacity to handle the real problems. A mobile-first dispatch system pushes all route details, patient information, and equipment requirements directly to technicians without requiring a phone call.
3. Missed Stops Are Discovered the Next Morning
When a technician skips a stop, either accidentally or due to time constraints, how quickly does your operation know? If the answer is "when we reconcile routes the next morning," every missed stop is a guaranteed reschedule. The patient waited all day. The physician's office may call wondering what happened. Your customer service team takes an angry call. And the missed stop now has to be squeezed into tomorrow's already full schedule.
Modern dispatch systems track stop completion in real time and alert dispatchers immediately when a stop is skipped or marked incomplete. This gives you a window to reassign the stop to another nearby technician, call the patient proactively, or adjust the route before the day ends.
4. You Have No Disruption Recovery Plan
Every day in DME field ops includes disruptions. A technician calls in sick. A vehicle breaks down. A patient cancels. An urgent delivery gets added at 11 AM. The question is whether your dispatch process can absorb these disruptions or whether each one triggers a cascade of manual phone calls and guesswork.
If a vehicle breakdown at 9 AM means your dispatcher spends the next hour on the phone manually reassigning stops, you're paying for that disruption twice: once in the lost productivity and again in the dispatcher's time to fix it. Intelligent dispatch systems can automatically redistribute affected stops to nearby technicians with available capacity and the right credentials, turning an hour of chaos into a five-minute adjustment.
5. Your Dispatchers Can't Take a Day Off
This is perhaps the most telling sign of all. If your dispatch operation depends entirely on the knowledge in one or two people's heads, you have a single point of failure. When that dispatcher is sick, on vacation, or leaves the company, the operation stumbles. Routes are less efficient. Credential mismatches increase. Technicians get confused. Patients get missed.
The knowledge that makes a great dispatcher effective, such as which techs are best in which neighborhoods, which patients need morning appointments, which payers require specific credentials, shouldn't live in someone's head. It should live in a system that anyone on the team can operate.
What to Do About It
If you recognized your operation in two or more of these signs, you're not alone. Most DME providers have grown their dispatch process organically over years, layering spreadsheets, phone calls, and tribal knowledge on top of each other. It works until it doesn't.
The fix isn't replacing your dispatchers. It's giving them tools that match the complexity of the job. Real-time visibility, automated route generation, credential-aware assignments, and instant disruption recovery aren't aspirational features. They're table stakes for any DME provider that wants to grow without proportionally growing dispatch headcount.
Great dispatchers are worth their weight in gold. But even the best dispatcher can't outperform a broken process. Give them the tools to succeed, and watch what happens.
About the Author

Adam Donaldson
Founder, CareLogix Health
Adam built CareLogix after years of implementing field operations systems at enterprise DME providers. He saw firsthand how fragmented tools, manual processes, and disconnected workflows cost branches hours every day and leak revenue that should have been captured. CareLogix is the platform he wished existed when he was on the implementation side.
Connect on LinkedIn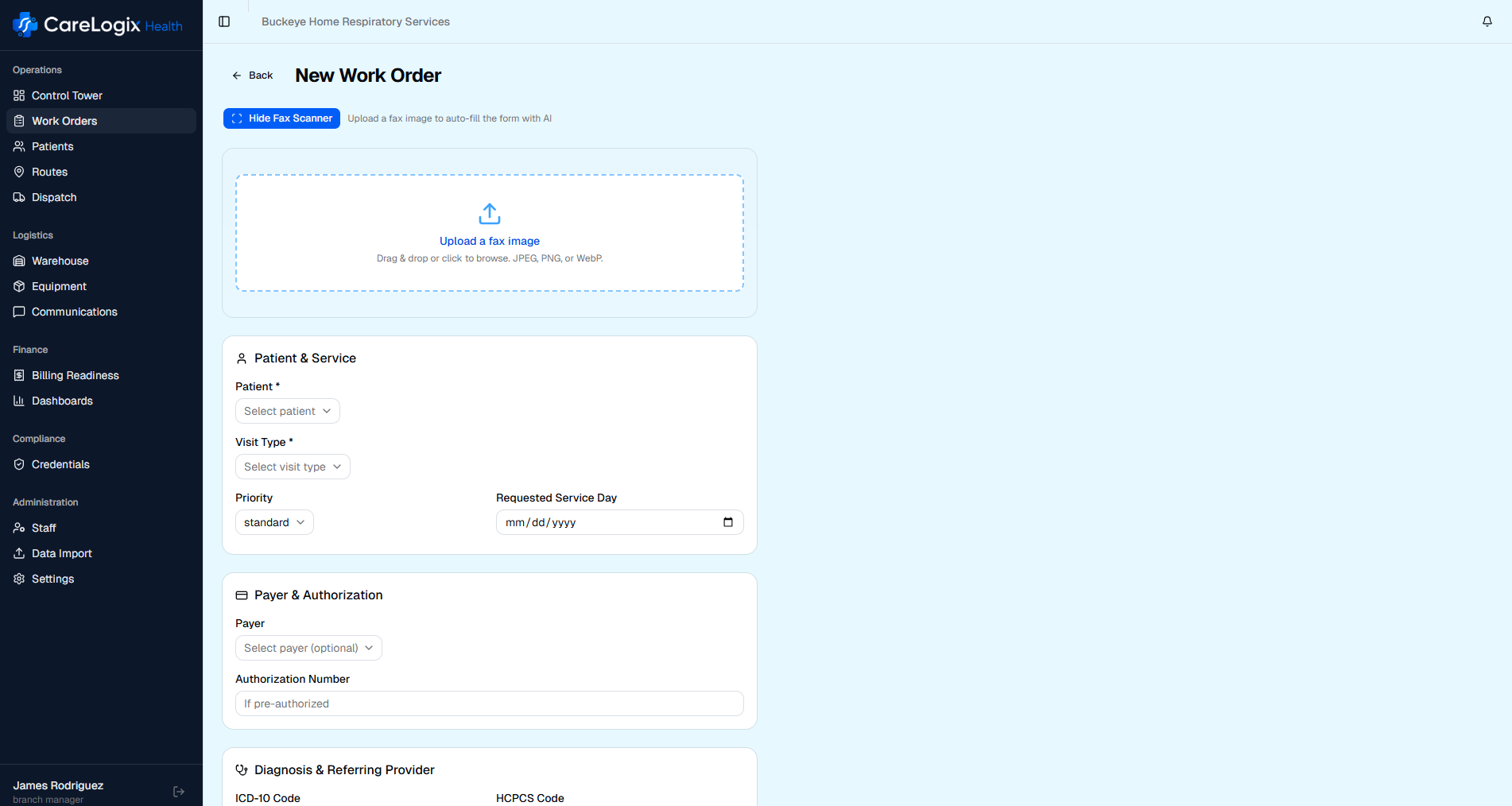
See CareLogix in Action
Schedule a 30-minute walkthrough and see how CareLogix manages the full work order lifecycle for DME providers like you.